Antibody Polyspecificity
How to Identify Off-Target Binding for Antibody-Directed Biotherapeutics
Home » Membrane Proteome Array » Antibody Polyspecificity – Identify Off-Target Liabilities
Antibody polyspecificity, also known as CDR-specific off-target binding, is a major concern for drug safety. In the clinic, off-target binding can cause adverse events and drug failures. It’s especially dangerous for targeted cell-killing modalities, such as CAR-T cell therapies, bispecifics, and antibody-drug conjugates (ADCs).
Read on to learn more about antibody polyspecificity, and how cell-based protein arrays are replacing older technologies for identifying off-target liabilities.
On this page:
Antibody Polyspecificity Is an Understudied Problem in Drug Development

For the full analysis of antibody polyspecificity in preclinical and clinical MAbs, with a review of the cell-based protein arrays for polyspecific off-target binding, as well as the limitations of TCR, see Norden et al 2024, mAbs 16, 1.
In conducting specificity screens using the Membrane Proteome Array (MPA), we’ve found that 33% of antibody-based drug candidates are polyspecific. But the problem isn’t restricted to preclinical lead candidates. In our analysis of 83 clinical MAbs, including currently approved and marketed drugs, 18% had off-target binding.
If the FDA requires specificity testing for antibody-based therapeutics, then why is the rate of off-target binding in clinical MAbs so high? It’s likely because of the reliance on a 40-year-old technique, tissue cross-reactivity (TCR) studies, which are failing to detect off-target binding. TCR has well-known limitations, and it lacks the sensitivity and other advantages of newer cell-based protein array platforms like the MPA.
Polyspecificity vs. Polyreactivity
Polyspecific off-target binding is distinct from polyreactivity*. Polyspecificity occurs through the antibody’s complementarity-determining region (CDR). It’s a “specific interaction with a discrete number of proteins which may or may not be related in terms of sequence or structural motifs.” Because so many off-target interactions have gone undetected, improved technologies—including cell-based protein arrays—are emerging for detecting polyspecificity and identifying off-targets for follow-up study.
In contrast, polyreactivity refers to general antibody “stickiness” through low-affinity, non-specific interactions across tissues. Polyreactivity is a well-known developability risk, and the assays for detecting it are well defined.
* The definitions here are from Cunningham et al., 2021; see the article for a full discussion on the topic.
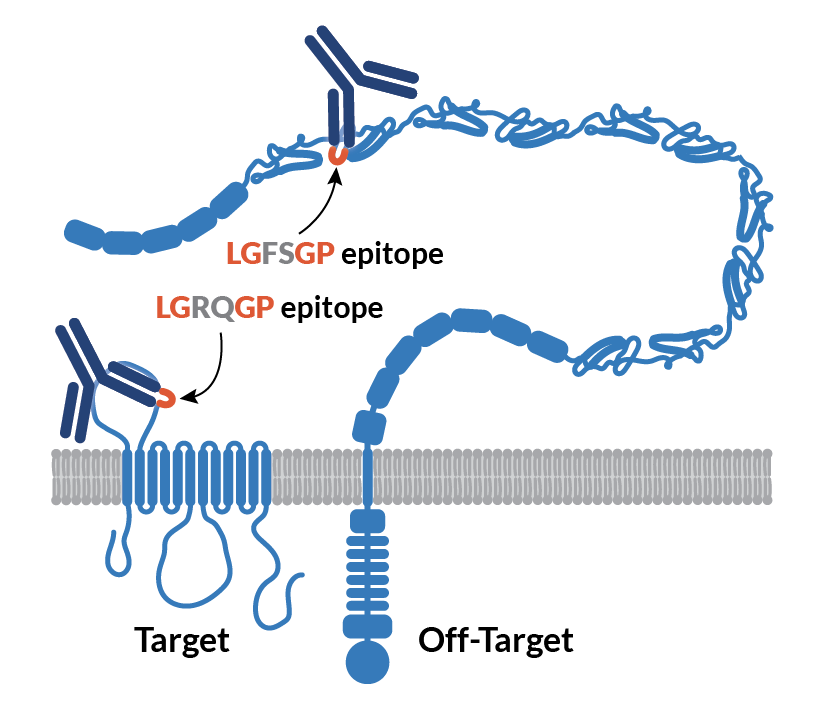
One mechanism for CDR-mediated antibody polyspecificity, as shown by epitope mapping. Even though the target and off-target have only 7% sequence identity, the two proteins share an LGXXGP epitope. (Graphic based on Norden et al., Fig. 6. For more details, see the case study How can a MAb cross-react with a completely unrelated protein?)
TCR Is Poor at Detecting Antibody Off-Targets
Tissue cross-reactivity (TCR) studies, first recommended by the FDA in 1983, are still commonly used for specificity testing—even though toxicologists say TCR results have no impact on development strategies for 95% of molecules (MacLachlan et al., 2021). Among their limitations, TCR studies are expensive, time consuming, and difficult to interpret. Most importantly, TCR studies don’t actually predict drug safety very well (Leach et al., 2010).
Cell-based protein arrays are a more sensitive, consistent, and accurate alternative to TCR. As the three case studies below demonstrate, the Membrane Proteome Array detects off-target cross-reactivity that TCR studies miss. And it does so at a lower cost, on a faster timeline, and with quantitative results.
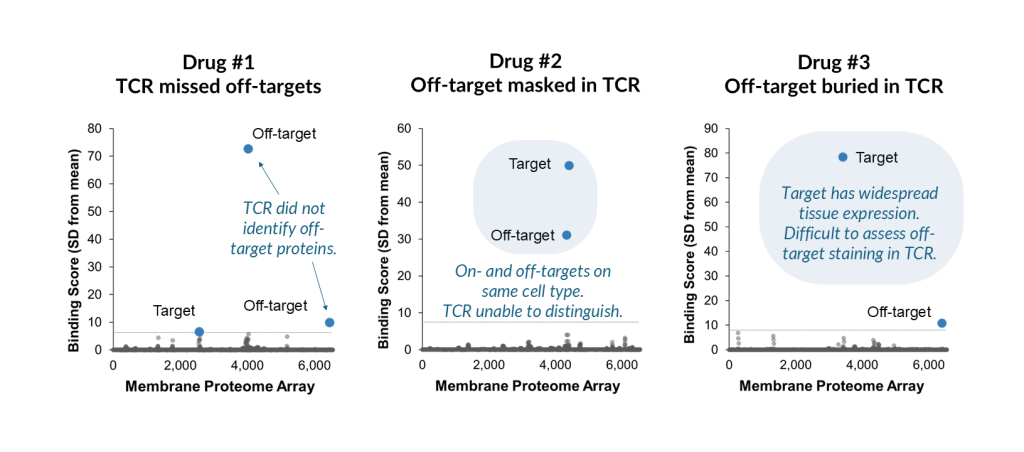
Graphics adapted from Norden et al., Fig. 8; see the article for a full description.
Our analysis of clinical MAbs (data from Norden et al., 2024) suggests that off-target binding is a major cause of drug attrition in the clinic—in part because TCR (the dominant screening method) is missing off-target interactions earlier in drug development. While off-target binding does not always produce adverse events, for example if the off-target is not accessible to the drug, our analysis suggests that MAbs without off-targets are much more successful in the clinic.
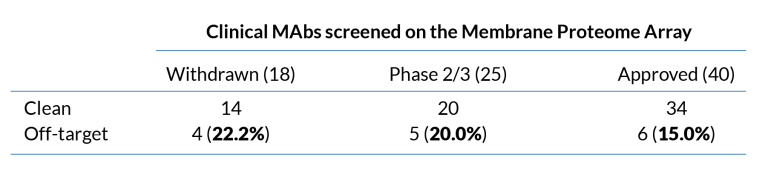
Based on Norden et al., table 2
Cell-Based Protein Arrays Identify Off-Targets and Predict Safety
The greatest limitation of tissue-based studies is that they cannot identify a specific molecular off-target—only the tissue in which it is expressed. In contrast, cell-based protein arrays, including the MPA, precisely identify protein off-targets. Knowing the identity of off-targets provides opportunities for follow-up studies into potential safety issues.
For MPA customers whose specificity screens return an off-target binding interaction, our Enhanced Binding Analysis service can inform next steps for continued development. This service includes statistical confirmation of off-target binding, the relative strength of the off-target interaction, and the epitope location and accessibility of the off-target.
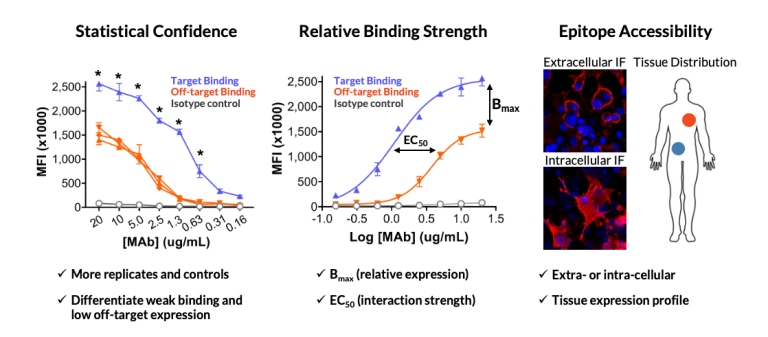
Integral Molecular’s Enhanced Binding Analysis service provides deeper statistical, biological, and molecular insights into off-targets identified on the Membrane Proteome Array.
The FDA Routinely Accepts MPA Specificity Data in IND Filings
Specificity testing is a critical component of safety assessment for all antibody-based therapeutics (see FDA Guidance Documents section, below). Over 100 IND filings with the FDA have already included MPA specificity data, in several cases without TCR data. Our expedited MPA+IND service, with additional reporting and quality parameters for supporting regulatory review, is available specifically for this purpose. And our ISO 9001-certified processes represent our ongoing commitment to quality.
For examples of programs that have used MPA data in regulatory submissions, see the following case studies:
The Membrane Proteome Array has already been used in >100 IND filings, and it is being evaluated by the FDA to become a qualified Drug Development Tool (DDT). The MPA was the first tool to be accepted into the FDA’s ISTAND program, in 2022, and it is the only cell-based protein array with an approved qualification plan. Learn more about ISTAND, ongoing improvements to the MPA, and what it means for the quality of your data.

Image credit, FDA
FDA Guidance Documents for Antibody Specificity Testing
The FDA, ICH, and other regulatory agencies provide guidance documents for evaluating specificity in biotherapeutics. Relevant FDA documents are linked below.
- Points to Consider in the Manufacture and Testing of Monoclonal Antibody Products for Human Use (February 1997). Page 30: “Appropriate newer technologies should be employed as they become available and validated.” Page 31: TCR is mentioned. Page 46: tissues that should be tested.
- S6(R1) Preclinical Safety Evaluation of Biotechnology-Derived Pharmaceuticals (May 2012). S6 addendum, page 10, Note 1: “Other technologies can be employed in place of [immunohistochemical] techniques to demonstrate target /binding site distribution.”
- Considerations for the Development of Chimeric Antigen Receptor (CAR) T Cell Products (January 2024). Page 21: “unintended targeting of other antigens expressed on healthy/normal tissue is a safety concern that may be evaluated using in vitro and/or in vivo studies.” Protein arrays are listed as an example.
Contact Us to Get a Quote and Start a Project
Featured Webinar
Redefining Antibody Specificity Profiling for IND
Webinar topics include:
- How the MPA can be used to rapidly and accurately identify potential off-target binding liabilities
- Ways MPA data support both lead selection and IND submissions, with a look at the advantages over tissue cross-reactivity studies
- The rapid progression of cell protein arrays towards FDA endorsement, including a deep dive into the inclusion in CAR-T development guidelines and qualification as an antibody Drug Development Tool